Chest Pain Emergencies in the ED
A high-yield guide and lecture supplement for emergency medicine learners
Chest pain is one of the most common complaints in emergency medicine, and one of the most consequential. Most patients with chest pain will not have acute coronary syndrome or another immediately life-threatening diagnosis. The challenge is finding the dangerous minority without indiscriminately testing everyone for everything.
This guide focuses on a practical emergency medicine approach:
Recognize instability. Consider the rapidly fatal diagnoses. Estimate pretest probability. Test intelligently. Treat before certainty when the situation demands it.
The following is a supplement to the in-person lecture delivered by Dr. Farzad. It is designed primarily for senior medical students rotating in emergency medicine and emergency medicine residents, but the principles apply broadly to acute care clinicians.
Jump to a specific section:
Framework · ACS / OMI · Pulmonary Embolism · Acute Aortic Syndrome · Tension Pneumothorax· Esophageal Rupture · Acute Chest Syndrome· Myopericardial Syndromes· Tamponade · Unstable Patient
Start with the Dangerous Minority of Chest Pain
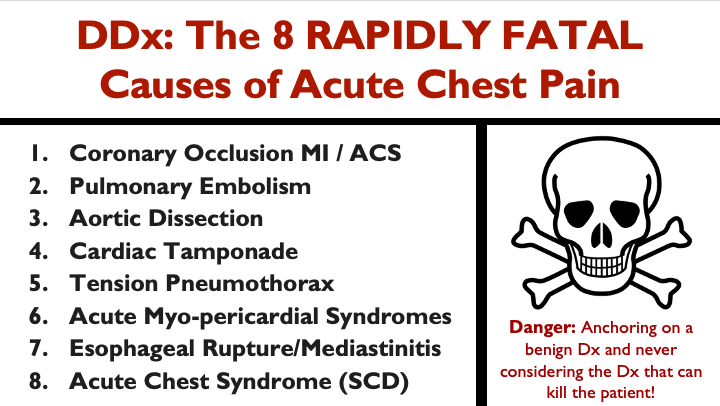
These eight diagnoses form the mental checklist that should run in the background whenever you evaluate acute chest pain. They are not equally common, and they will not all be plausible in every patient. The point is not to test every patient for all eight. The point is to avoid premature closure before you have seriously considered the diagnoses where delay can be catastrophic.
The danger is anchoring on a benign diagnosis and never seriously considering the diagnosis that can kill the patient.

Most patients who present to the ED with chest pain ultimately receive a nonspecific or nonischemic diagnosis. ACS accounts for only about 5% of presentations, pulmonary embolism roughly 0.5%, and acute aortic syndromes are even less common. But rarity does not make these diagnoses unimportant, it makes them easier to miss.
Rare + lethal + time-sensitive is exactly why structured thinking matters.
The central task in emergency chest pain evaluation is therefore not to ask whether every dangerous diagnosis is possible. Almost anything is possible. The better question is: How likely is each diagnosis in this patient, and what would move me to test or treat?
Think in Probabilities, Not Possibilities
One of the biggest differences between novice and expert clinical reasoning is the transition from asking, “Could this be PE?” to asking, “How likely is PE in this patient, and what information would meaningfully move that probability up or down?”
Almost anything could be something. Possibility alone is not a rational reason to test. The better approach is to estimate pretest probability, identify the findings that modify it, and use testing only when it can meaningfully change management.
Pretest probability is your starting estimate before the next test. It comes from the symptom story, trajectory, age, comorbidities, relevant risk factors, vital signs, examination, ECG, and POCUS when clinically appropriate.
The estimate is dynamic. New information should change it. A reassuring finding may lower probability; a high-risk feature may raise it substantially.
The question is not simply whether a diagnosis is possible. The question is whether it is probable enough to justify testing, treatment, or both.
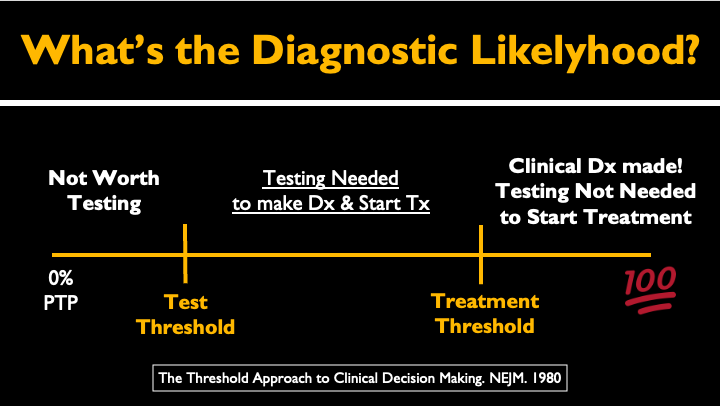
The threshold model is one of the most useful ways to understand diagnostic decision-making.
Below the test threshold
The probability of disease is low enough that testing is more likely to create harm than benefit through false positives, incidental findings, radiation, contrast exposure, unnecessary downstream procedures, or avoidable anxiety.
Between the test and treatment thresholds
Additional testing is useful because the result may meaningfully change management.
Above the treatment threshold
The probability and consequences of disease are high enough that treatment should begin before every confirmatory step is complete.
Examples include immediate decompression of an unstable tension pneumothorax, emergent reperfusion when acute coronary occlusion is apparent, and anti-impulse therapy while definitive imaging is arranged for suspected acute aortic syndrome.
Not every dangerous diagnosis requires certainty before action. The more unstable the patient and the more time-sensitive the disease, the less diagnostic certainty may be available before treatment must begin.
Key reference
Pauker SG, Kassirer JP. The Threshold Approach to Clinical Decision Making. N Engl J Med. 1980. PMID: 7366635.
The next step is understanding how history and examination findings modify those probabilities. They are not binary answers. They are probability tools.
The History Is a Probability Tool
History and physical examination findings are not yes-or-no answers. They are probability modifiers. Some findings increase the likelihood of disease, some decrease it, and very few are powerful enough to rule a dangerous diagnosis in or out by themselves.
The goal is not to collect every possible symptom. It is to ask the questions that meaningfully change pretest probability.
A symptom that increases likelihood does not prove disease. A symptom that decreases likelihood does not rule it out.
Exertional pressure with diaphoresis and radiation should increase concern for ACS. Pleuritic pain with unexplained dyspnea and tachycardia should raise concern for PE. Abrupt severe pain with syncope or a neurologic deficit should raise concern for acute aortic syndrome. The value of the history is in how these features change probability in the specific patient in front of you.
Ask the right questions in the right way
Start open-ended. Let the patient describe what happened before converting the history into a checklist of yes-or-no questions. Then clarify onset, location, duration, evolution, provoking factors, relieving factors, associated symptoms, and relevant preceding events.
Listen first. Interrogate the details second.
Essential reading
Does This Patient With Chest Pain Have Acute Coronary Syndrome?
Fanaroff AC, Rymer JA, Goldstein SA, et al. The Rational Clinical Examination Systematic Review. JAMA. 2015. PMID: 26547467.
This is the most important focused reading for this section and one I strongly recommend every emergency medicine learner read. It reviews which elements of the history, examination, and ECG actually change the probability of ACS and highlights the limitations of relying on any single chest-pain feature.
It is especially useful for understanding why findings such as diaphoresis, radiation, exertional symptoms, pleuritic pain, positional pain, and reproducible tenderness should be treated as probability modifiers rather than binary answers.
[Read the full text] · [View on PubMed]
A Favorite Reference to Browse
The Rational Clinical Examination: Evidence-Based Clinical Diagnosis. JAMA / McGraw-Hill.
This is one of my favorite medical references and one I have recommended to learners for years. It is not meant to be read front to back. Think of it as a reference to browse through when you want to understand which elements of the history and physical examination actually matter for a specific diagnosis.
The broader Rational Clinical Examination series deserves a special mention here. It has helped shape the way many clinicians think about diagnostic reasoning by asking a simple but powerful question:
How much does this finding actually change the probability of disease?
That is exactly the kind of thinking we want to bring to the bedside.
Foundational Guideline
2021 AHA/ACC Multisociety Guideline for the Evaluation and Diagnosis of Chest Pain
Gulati M, Levy PD, Mukherjee D, et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain. PMID: 34709879.
This is the broad foundational guideline for contemporary chest-pain evaluation. It emphasizes that chest pain may include pressure, tightness, dyspnea, fatigue, epigastric discomfort, and pain in the arm, jaw, back, or other locations. It also supports the use of high-sensitivity troponin, serial ECGs when symptoms persist or evolve, structured clinical decision pathways, and avoiding unnecessary testing in appropriately selected low-risk patients.
[Read the full guideline] · [View on PubMed]
The same probability-based approach applies to every dangerous diagnosis in this guide. We will start with the most common of them: acute coronary syndrome and coronary occlusion MI.
End of this Section. Jump back to Top for section menu , or continue reading…
Coronary Occlusion MI and Acute Coronary Syndrome
Acute coronary syndrome is the most common of the rapidly fatal diagnoses in this guide, but the emergency physician’s job is not simply to decide whether a patient meets traditional STEMI criteria.
An acutely occluded coronary artery may present without classic STEMI criteria. The more important question is:
Is there evidence of acute coronary occlusion or another high-risk ischemic pattern that requires immediate action?
Look for:
A single ECG is only a snapshot. When symptoms persist, recur, or evolve, repeat the ECG.
Serial ECGs are critically important. They are a diagnostic and treatment tool.
A normal initial troponin also does not protect a patient with evolving coronary occlusion. The ECG, symptoms, timing, trajectory, and biomarker trend must be interpreted together.
Because ACS and OMI deserve a much deeper discussion than can fit into this guide, this section is intentionally focused. See my the dedicated ACS / Occlusion MI lecture guide (coming soon) and related ECG STAT post on Occlusion MI: STEMI Criteria & Beyond for a more complete review.
Features That Make ACS More Likely
Several associated features should raise the probability of ACS:
Diaphoresis. Radiation. Vomiting. Exertional symptoms.
These findings are not diagnostic by themselves, but when they occur together, especially in a compatible clinical context—they should meaningfully increase concern.
Autonomic symptoms such as diaphoresis and vomiting are particularly important warning features. Radiation to the arm, jaw, neck, or back and symptoms provoked by exertion should also increase suspicion.
Do not dismiss ACS because the patient is young, female, diabetic, lacks traditional risk factors, or has a normal initial troponin.
Unstable angina still exists in the high-sensitivity troponin era, although it is less common than it once appeared to be. A patient may have ACS despite negative biomarkers and a normal or nonspecific ECG, particularly when the clinical history is strongly ischemic or symptoms are recurrent or crescendoing.
Features That Make ACS Less Likely
Certain characteristics lower the probability of ACS:
Sharp. Positional. Pleuritic. Reproducible.
But none of these findings alone excludes ACS.
A patient can have chest wall tenderness and still have myocardial infarction. A patient can describe pleuritic discomfort and still have ACS. Positional pain may suggest pericarditis, but the ECG and broader clinical picture still matter.
One reassuring feature should never be allowed to erase multiple high-risk findings.
Do not use a single low-risk historical characteristic to override:
a concerning ECG
exertional or crescendo symptoms
recurrent ischemic discomfort
hemodynamic instability
acute heart failure
ventricular arrhythmia
strong overall clinical concern for ACS
HEART Score: A Tool, Not a Disposition Decision
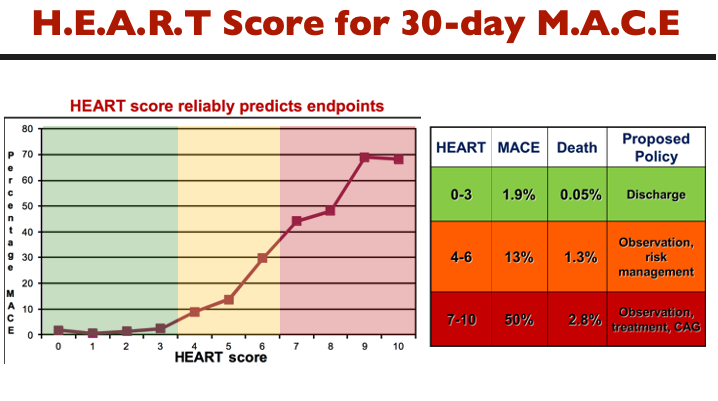
The HEART score can help structure short-term risk stratification, but it should support clinical judgment rather than replace it.
The most subjective component is the History score.
A practical approach is to ask:
Is this history primarily ischemic, mixed or unclear, or primarily nonischemic?
If you cannot justify the history score in one sentence using concrete features from the case, the score is probably not reliable.
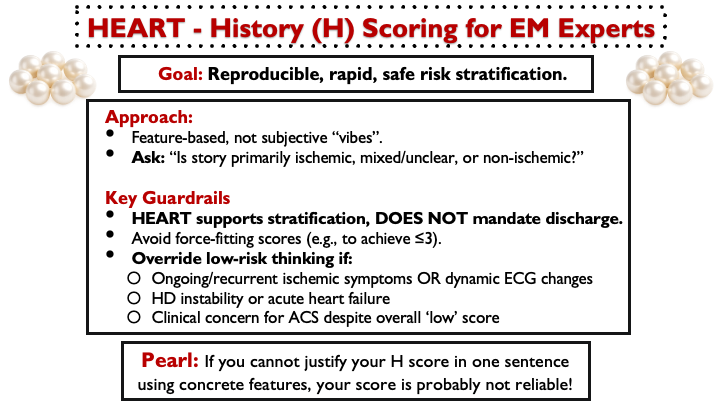
A few guardrails
Do not force-fit the score to achieve a HEART score of 3 or less.
A low score does not override ongoing or recurrent ischemic symptoms.
Dynamic ECG changes should immediately override low-risk thinking.
Hemodynamic instability or acute heart failure should not be squeezed into a routine low-risk pathway.
Persistent clinical concern for ACS matters, even when the calculated score appears reassuring.
HEART supports risk stratification. It does not mandate discharge.
Scoring the HEART history
-
The history is predominantly ischemic, particularly when several classic features are present without a convincing alternative diagnosis:
substernal pressure, heaviness, or tightness
exertional or stress-related onset
crescendo pattern
radiation to the arm, jaw, or neck
diaphoresis, vomiting, or dyspnea
symptoms similar to prior angina or MI
A normal initial ECG or troponin should not erase a strongly ischemic history.
Active, recurrent, or crescendo symptoms deserve particular attention.
-
The history contains some ischemic features but is mixed, incomplete, or not convincing enough to call highly suspicious.
Examples include:
one typical ischemic feature mixed with atypical elements
nonclassic location or quality with concerning associated symptoms
a limited historian in whom ischemia remains plausible
Uncertainty should lead to better evaluation—not false reassurance.
-
The history is primarily nonischemic.
Examples include:
pleuritic pain
positional pain
reproducible tenderness
very brief pain lasting seconds
prolonged unchanged discomfort without evolution
symptoms that closely track with a convincing GI, musculoskeletal, respiratory, or other alternative diagnosis
A score of zero does not mean zero risk. It means the history itself is not ischemic.
Low-risk disposition still depends on the ECG, troponin pathway, clinical trajectory, and absence of other high-risk features.
Essential Reading
2022 ACC Expert Consensus Decision Pathway on Acute Chest Pain in the ED
Kontos MC, de Lemos JA, Deitelzweig SB, et al. 2022 ACC Expert Consensus Decision Pathway on the Evaluation and Disposition of Acute Chest Pain in the Emergency Department. PMID: 36241466.
This is probably the single most operationally useful chest-pain document for emergency clinicians. It goes beyond traditional STEMI criteria, recognizes several high-risk ischemic and STEMI-equivalent patterns, emphasizes serial ECGs and posterior leads when indicated, and provides practical guidance for high-sensitivity troponin pathways and disposition.
For this guide, this is the most important ACS reference.
[Read the full text] · [View on PubMed]
2025 ACC/AHA/ACEP/NAEMSP/SCAI Guideline for Acute Coronary Syndromes
Rao SV, et al. 2025 ACC/AHA/ACEP/NAEMSP/SCAI Guideline for the Management of Patients With Acute Coronary Syndromes. PMID: 40013746.
The most current major U.S. ACS guideline and particularly relevant to emergency medicine because ACEP participated in its development. It should serve as the major contemporary reference for ACS management, reperfusion, antithrombotic therapy, and the unstable patient.
[Read the full guideline] · [View on PubMed]
HEART Score Systematic Review and Meta-analysis
Laureano-Phillips J, Robinson RD, Aryal S, et al. HEART Score Risk Stratification of Low-Risk Chest Pain Patients in the Emergency Department: A Systematic Review and Meta-analysis. Ann Emerg Med. 2019. PMID: 30718010.
Useful for understanding the performance and limitations of HEART-based risk stratification across a large body of studies.
[Read the full text] · [View on PubMed]
End of this Section. Jump back to Top for section menu , or continue reading…
Acute Pulmonary Embolism
Pulmonary embolism is fundamentally a probability diagnosis. The challenge is not to test every patient with chest pain or dyspnea. It is to identify who is sufficiently low risk to stop, who needs a D-dimer, who needs imaging, and who is unstable enough to require immediate treatment.
Consider PE when the presentation includes unexplained dyspnea, pleuritic chest pain, tachypnea, unexplained tachycardia, hypoxemia, unilateral leg swelling, syncope, or signs of acute right-heart strain or obstructive shock.
PE severity is determined by the patient’s clinical physiology and risk of deterioration, not simply by clot size or how dramatic the CT looks. The 2026 AHA/ACC guideline introduces Acute PE Clinical Categories A–E, ranging from incidental/asymptomatic PE to cardiopulmonary failure.
For emergency clinicians, the key distinction is whether the patient is stable, showing evidence of RV stress or deterioration, or already in cardiopulmonary failure.
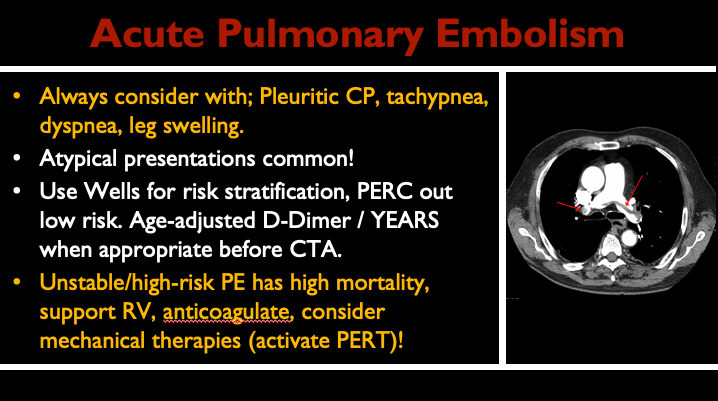
The diagnostic approach begins with pretest probability. PERC is not a screening tool for every patient with chest pain or dyspnea. It is a rule-out strategy for patients already judged to have a sufficiently low pretest probability of PE.
In appropriate patients, structured probability assessment, age-adjusted D-dimer, or the YEARS strategy can help determine who needs imaging and who can safely avoid unnecessary CTPA.
A practical way to think about PE testing
Very low probability
Consider PERC only when the patient is already clinically very low risk.
Low or intermediate probability
Use a validated pathway such as Wells-based assessment, age-adjusted D-dimer, or YEARS when appropriate.
High probability
Proceed directly to definitive imaging when clinically feasible rather than relying on D-dimer testing.
Hemodynamically unstable
This is no longer simply a diagnostic-workup problem. Think obstructive shock, support the right ventricle, use bedside echocardiography when it can rapidly answer a focused question, and move early toward a reperfusion strategy.
The diagnostic pathway for a stable patient with possible PE is very different from the resuscitation pathway for a patient in obstructive shock.
Common Pitfalls
In high-risk PE, the immediate priorities are hemodynamic support, anticoagulation when appropriate, and rapid consideration of reperfusion. Depending on the patient, contraindications, local resources, and institutional expertise, options may include systemic thrombolysis, catheter-based therapy, surgical embolectomy, or ECMO as rescue or bridge therapy in selected cases.
Be especially cautious with intubation. Loss of sympathetic tone and initiation of positive-pressure ventilation can precipitate cardiovascular collapse in patients with severe RV failure and obstructive shock.
Related ECG STAT Learning & Essential Reading
S1Q3T3 Pattern (ECG STAT)
A classic but frequently overinterpreted ECG pattern. S1Q3T3 reflects acute right-heart strain and is not specific for pulmonary embolism.
ECG Findings in Pulmonary Embolism (ECG STAT)
Review the broader spectrum of ECG abnormalities associated with acute PE, including sinus tachycardia, right-axis deviation, right bundle branch block, anterior and inferior T-wave inversion, and other manifestations of acute RV strain.
2026 AHA/ACC Multisociety Guideline for Acute Pulmonary Embolism
Creager MA, et al. 2026 AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM Guideline for the Evaluation and Management of Acute Pulmonary Embolism in Adults. PMID: 41712898.
This is the primary contemporary guideline for this section and the most important overall PE reference for U.S. emergency medicine learners. It covers clinical probability assessment, diagnostic testing, severity classification, acute management, hospitalization decisions, anticoagulation, reperfusion strategies, advanced therapies, PERT systems, and follow-up.
A major update is the introduction of the AHA/ACC Acute PE Clinical Categories A–E, designed to classify patients according to clinical severity and risk of adverse outcomes rather than relying solely on older terms such as massive and submassive PE. The guideline also supports early multidisciplinary PE response systems and provides contemporary recommendations for systemic thrombolysis, catheter-based therapy, mechanical thrombectomy, and surgical embolectomy in appropriately selected patients.
[Read the full guideline] · [View on PubMed]
Prospective Multicenter Evaluation of the Pulmonary Embolism Rule-Out Criteria
Kline JA, Courtney DM, Kabrhel C, et al. PMID: 18318689.
Essential reading for understanding what PERC was designed to do, and equally importantly, when it should not be used.
[Read the full text] · [View on PubMed]
The YEARS Algorithm for Suspected Pulmonary Embolism
van der Pol LM, et al. PMID: 29431911.
A practical diagnostic strategy using three clinical items and variable D-dimer thresholds to reduce unnecessary CTPA in appropriately selected patients.
[Read the full text] · [View on PubMed]
End of this Section. Jump back to Top for section menu , or continue reading…
Acute Aortic Syndrome
Acute aortic syndrome is uncommon—but when missed, the consequences can be catastrophic. It is an umbrella term that includes aortic dissection, intramural hematoma, and penetrating atherosclerotic ulcer.
The classic teaching of sudden tearing chest pain radiating to the back is memorable, but real presentations are often less obvious. Patients may present with chest, back, or abdominal pain, syncope, neurologic deficits, limb ischemia, hypotension, or a new murmur of aortic regurgitation.
Do not wait for the classic hypertensive patient with tearing chest-to-back pain. Acute aortic syndrome may present with normal blood pressure, hypotension, isolated neurologic findings, or pain outside the chest.
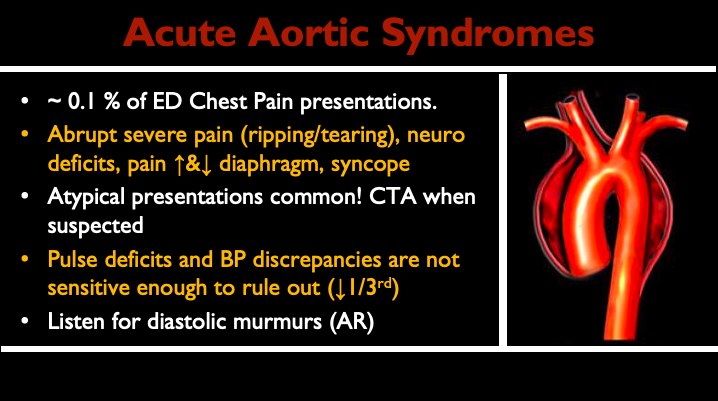
The history and examination should modify pretest probability, but no single absent finding safely excludes the diagnosis. Pulse deficits, inter-arm blood pressure differences, and aortic regurgitation are important when present, but their absence should not falsely reassure you.
When suspicion is meaningful, CTA is generally the definitive first-line diagnostic study in a hemodynamically stable patient.
When to Think of Acute Aortic Syndrome
Features that should increase concern include:
abrupt onset of severe pain
maximal intensity at onset
chest, back, or abdominal pain
syncope
focal neurologic deficit
spinal cord ischemia
limb ischemia
pulse deficit
unexplained hypotension or shock
new aortic regurgitation murmur
known aortic disease or other high-risk predisposing conditions
Pain that moves above and below the diaphragm, neurologic symptoms accompanying pain, or unexplained malperfusion should immediately raise concern for aortic catastrophe.
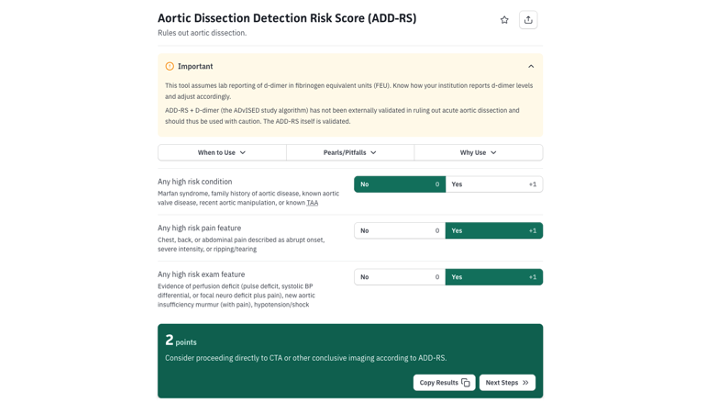
The Aortic Dissection Detection Risk Score, or ADD-RS, provides a structured way to think about pretest probability using three domains:
high-risk predisposing conditions
high-risk pain features
high-risk examination findings
The main value of the ADD-RS is not that it replaces clinical judgment. Its value is that it forces us to deliberately consider the findings that meaningfully change probability.
A score of zero does not mean zero risk. Use the ADD-RS to structure thinking, not to override a concerning patient.
A Practical Way to Think About Testing
Low clinical probability
A low ADD-RS in a patient without other concerning features may support avoiding unnecessary advanced imaging.
Intermediate probability
Consider whether D-dimer has a role within a validated diagnostic strategy and in the appropriate clinical context.
High probability
Do not rely on D-dimer to rescue a high-risk patient. Proceed to definitive imaging when feasible.
Hemodynamically unstable
The pathway changes completely. Use bedside imaging when it can immediately answer a focused question, obtain surgical involvement early, and do not delay resuscitative treatment while pursuing diagnostic perfection.
The diagnostic strategy should follow the patient’s probability and physiology, not a score alone.
Treat Shear While You Diagnose
When acute aortic syndrome is strongly suspected, the immediate goal is to reduce aortic wall stress while definitive imaging and specialty involvement are arranged.
In most patients requiring anti-impulse therapy:
reduce heart rate first with an IV beta-blocker
control blood pressure while preserving organ perfusion
add vasodilator therapy only after adequate rate control when needed
A practical hemodynamic target is generally a heart rate around 60–80 beats/minute and systolic blood pressure below 120 mm Hg when tolerated, with treatment individualized to maintain adequate end-organ perfusion.
Beta-block first. Do not reflexively give a vasodilator before controlling heart rate, because increasing reflex tachycardia may worsen shear forces.
Common Pitfalls
Do not rule out acute aortic syndrome because the patient is normotensive.
Do not rely on the absence of pulse deficits or inter-arm blood pressure differences.
Do not assume every dissection presents with tearing chest-to-back pain.
Do not let a low ADD-RS override a truly concerning presentation.
Do not delay surgical consultation in suspected proximal aortic catastrophe while waiting for every detail of the workup to be complete.
Essential Reading
2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease
Isselbacher EM, Preventza O, Hamilton Black J III, et al. 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease. PMID: 36322642.
This is the primary contemporary U.S. guideline for acute aortic syndrome and the most important reference for this section. It covers diagnosis, imaging, anti-impulse therapy, surgical indications, and management across the spectrum of aortic disease.
[Read the full guideline] · [View on PubMed]
Aortic Dissection Detection Risk Score
Rogers AM, Hermann LK, Booher AM, et al. Sensitivity of the Aortic Dissection Detection Risk Score, a Novel Guideline-Based Tool for Identification of Acute Aortic Dissection at Initial Presentation. PMID: 21555704.
This study is foundational for understanding the ADD-RS and how the score was designed to identify high-risk clinical features.
ADD-RS With D-Dimer
Tsutsumi Y, Tsujimoto Y, Takahashi S, et al. Accuracy of the Aortic Dissection Detection Risk Score Alone or With D-Dimer: A Systematic Review and Meta-analysis. PMID: 31970996.
Useful for understanding the strengths and limitations of combining clinical probability assessment with D-dimer in selected patients.
Acute aortic syndrome is a classic example of why emergency medicine depends on careful history, probability assessment, and recognition of high-risk physiology. The next emergency can deteriorate even faster and may require treatment before imaging is obtained: tension pneumothorax.
End of this Section. Jump back to Top for section menu , or continue reading…
Tension Pneumothorax
Tension pneumothorax is a clinical diagnosis in the unstable patient. When the physiology and examination fit, treatment should not wait for chest radiography.
Think about it especially in a patient with:
hypotension
severe hypoxemia
peri-arrest physiology
unilateral loss or marked reduction of breath sounds
recent trauma
positive-pressure ventilation
The more unstable the patient, the less acceptable it is to delay decompression for diagnostic certainty.
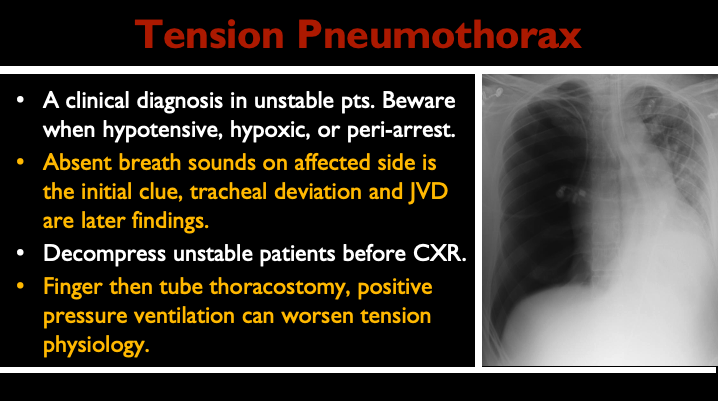
The classic teaching of tracheal deviation and jugular venous distention is memorable, but both are often late and unreliable. In the unstable patient, the earlier clue may simply be a compatible presentation with unilateral absent or markedly reduced breath sounds.
Positive-pressure ventilation can rapidly worsen tension physiology by further increasing intrathoracic pressure and reducing venous return.
Do not wait for the full textbook picture before acting.
What Changes Management?
Unstable patient with suspected tension pneumothorax
Immediate decompression is indicated. Imaging should not delay treatment.
Stable patient with suspected pneumothorax
Imaging can help confirm the diagnosis and define the size and extent of the pneumothorax.
Patient requiring positive-pressure ventilation
Maintain a low threshold for concern because tension physiology can worsen rapidly after induction or initiation of positive-pressure ventilation.
Common Pitfalls
Do not wait for tracheal deviation.
Do not rely on jugular venous distention being present.
Do not delay decompression for chest radiography in an unstable patient when the diagnosis is clinically apparent.
Do not forget that positive-pressure ventilation can abruptly worsen obstructive physiology.
Treatment Pearl
In an unstable patient, the immediate goal is rapid decompression. Needle decompression can temporize, but finger thoracostomy and tube thoracostomy provide more definitive pleural access when appropriate and feasible.
The resuscitation principle is simple: treat the physiology first.
Suggested Reading
2023 British Thoracic Society Guideline for Pleural Disease
Roberts ME, Rahman NM, Maskell NA, et al. Thorax. 2023. PMID: 37553157
A contemporary evidence-based guideline covering pneumothorax and broader pleural disease management. For this guide, its main value is providing the broader pneumothorax framework around the immediately unstable patient.
[Read the full guideline] · [View on PubMed]
Esophageal rupture is much rarer, but the same principle applies: the diagnosis is uncommon, time-sensitive, and dangerous when missed.
End of this Section. Jump back to Top for section menu , or continue reading…
Esophageal Rupture and Mediastinitis
Esophageal rupture is rare, but when missed it can be catastrophic. The diagnosis is easy to overlook because the presentation can overlap with more common causes of chest pain, sepsis, or pleural disease.
Think beyond the classic story of forceful vomiting. Esophageal perforation can also follow:
endoscopy or other instrumentation
food impaction
trauma
severe retching
other iatrogenic injury
The danger is delayed recognition. The longer the perforation persists, the greater the risk of mediastinal contamination, sepsis, shock, and death
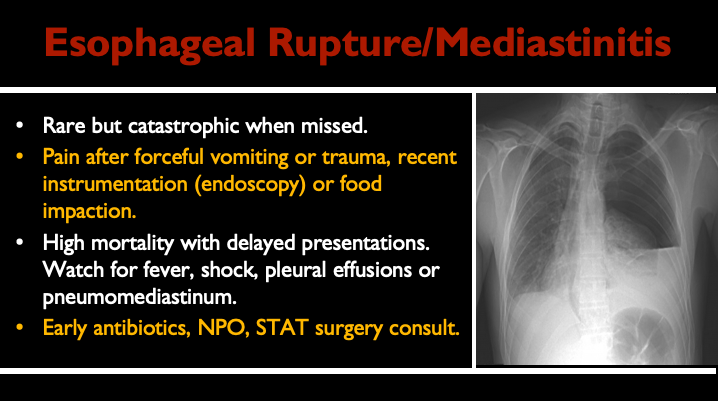
The classic presentation is severe chest pain after forceful vomiting, but the absence of that history does not exclude the diagnosis.
As the disease progresses, patients may develop:
fever
tachycardia
shock
pleural effusion
pneumomediastinum
subcutaneous emphysema
systemic toxicity
Subcutaneous emphysema is memorable, but it is not required. Many patients are diagnosed because someone considered esophageal perforation before the presentation became obvious.
Do not wait for the complete textbook picture.
When to Think of Esophageal Rupture
Consider the diagnosis when severe chest or upper abdominal pain follows:
forceful vomiting or retching
recent endoscopy or instrumentation
food impaction
trauma
other esophageal injury
Also consider it in a toxic patient with unexplained chest pain, pleural effusion, pneumomediastinum, or sepsis without a clear source.
What Changes Management?
Clinical suspicion should trigger early imaging and urgent specialist involvement.
Management typically includes:
NPO status
broad-spectrum antimicrobial therapy
aggressive resuscitation when needed
urgent surgical and/or gastroenterology consultation
source control tailored to the location, size, timing, and cause of the perforation
The most important emergency medicine contribution is early recognition and rapid escalation.
Common Pitfalls
Do not assume Boerhaave syndrome requires a textbook history of repeated vomiting followed by dramatic chest pain.
Do not wait for subcutaneous emphysema.
Do not dismiss pleural effusion or pneumomediastinum as incidental in a compatible presentation.
Do not delay antibiotics and specialist involvement while waiting for perfect diagnostic certainty.
Suggested Reading
Esophageal Emergencies: WSES Guidelines
Chirica M, Kelly MD, Siboni S, et al. World Journal of Emergency Surgery. 2019. PMID: 31164915
This is the key guideline-level reference for esophageal perforation and other esophageal emergencies. It covers diagnosis, imaging, antimicrobial therapy, operative and nonoperative management, and the importance of early recognition and source control.
[Read the full guideline] · [View on PubMed]
The next diagnosis is unique to patients with sickle cell disease, but it belongs on any chest pain differential when the clinical context fits: acute chest syndrome.
End of this Section. Jump back to Top for section menu , or continue reading…
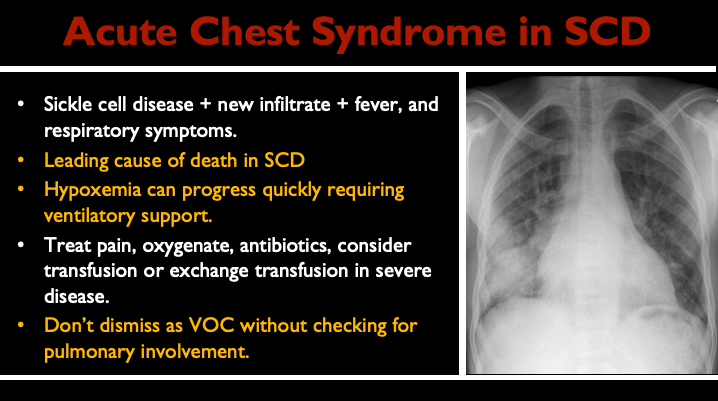
Acute Chest Syndrome in Sickle Cell Disease
Chest pain in a patient with sickle cell disease should never automatically be attributed to uncomplicated vaso-occlusive pain. Acute chest syndrome can progress rapidly and remains one of the most important life-threatening complications of sickle cell disease.
Think about acute chest syndrome when a patient with sickle cell disease has a new pulmonary infiltrate together with compatible clinical features such as:
fever
chest pain
cough
dyspnea
tachypnea
hypoxemia
The key danger is progression. A patient who initially appears relatively well can deteriorate quickly.
Acute chest syndrome is not a single-pathway disease. Infection, pulmonary infarction, fat embolism, hypoventilation, atelectasis, and other mechanisms may contribute, often in combination.
The emergency medicine priorities are early recognition, close reassessment, treatment of hypoxemia, appropriate analgesia, antibiotics, and prevention of further pulmonary compromise. Incentive spirometry is particularly important in patients admitted with vaso-occlusive pain because splinting and hypoventilation can contribute to development or progression of acute chest syndrome.
Do not dismiss worsening chest pain, new oxygen requirement, or respiratory symptoms as “just pain crisis.”
What Changes Management?
Hypoxemia or increasing oxygen requirement
This should immediately raise concern for progression and the need for closer monitoring and escalation of care.
New infiltrate with compatible symptoms
Treat as acute chest syndrome rather than uncomplicated vaso-occlusive pain alone.
Respiratory deterioration, worsening anemia, multilobar disease, or other severe features
Early hematology involvement and consideration of transfusion become increasingly important.
Severe or rapidly progressive disease
Exchange transfusion may be required in selected patients. The decision depends on severity, trajectory, oxygenation, hemoglobin level, and overall physiology rather than the diagnosis alone.
Common Pitfalls
Do not label all chest pain in sickle cell disease as uncomplicated vaso-occlusive pain.
Do not wait for profound hypoxemia before recognizing progression.
Do not assume every patient with acute chest syndrome needs immediate transfusion—but do not delay escalation when severe features are developing.
Do not overlook incentive spirometry in patients hospitalized with vaso-occlusive pain or acute chest syndrome
Practical Treatment Priorities
Management commonly includes:
appropriate analgesia
oxygen for hypoxemia
antibiotics
incentive spirometry
careful fluid management
transfusion when clinically indicated
exchange transfusion for selected severe or progressive cases
The exact treatment plan should follow the patient’s severity and trajectory rather than a one-size-fits-all checklist.
The emergency physician’s job is to recognize progression early and escalate before respiratory failure becomes obvious.
Essential Reading
2025 Guidelines for the Management of Emergencies and Critical Illness in Sickle Cell Disease
Mekontso Dessap A, et al. Guidelines for the Management of Emergencies and Critical Illness in Pediatric and Adult Patients With Sickle Cell Disease. 2025. PMID: 40439782.
This is the most current high-level guideline for emergency and critical illness management in sickle cell disease and directly addresses acute chest syndrome, transfusion therapy, escalation of care, and other major complications. For this section, it should be the primary reference.
[Read the full guideline] · [View on PubMed]
Acute chest syndrome is a disease in which deterioration may be initially subtle. The next group of disorders can be equally deceptive, ranging from benign-appearing pericarditis to fulminant myocarditis with arrhythmia, heart failure, or shock.
End of this Section. Jump back to Top for section menu , or continue reading…
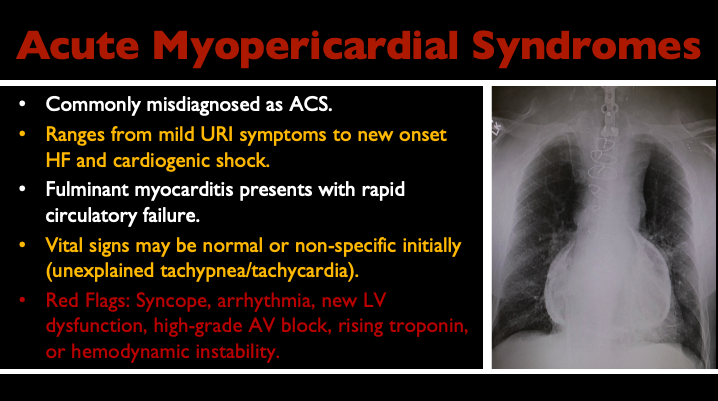
Acute Myopericardial Syndromes
Inflammatory myocardial and pericardial disease exists on a spectrum. At one end is uncomplicated acute pericarditis. At the other is fulminant myocarditis with malignant arrhythmia, severe ventricular dysfunction, cardiogenic shock, or conduction disease.
The emergency medicine challenge is recognizing the patient who initially looks relatively well but has evidence of myocardial involvement or a high-risk trajectory.
Do not assume that chest pain, ST elevation, and a positive troponin automatically mean ACS, or that every case of presumed pericarditis is benign.
Myocarditis can mimic many other emergency presentations, including:
acute coronary syndrome
acute heart failure
ventricular or supraventricular arrhythmia
high-grade AV block
syncope
cardiogenic shock
Vital signs may initially be normal or nonspecific. Unexplained tachycardia, tachypnea, new conduction disease, ventricular dysfunction, or a rising troponin should make you look beyond uncomplicated pericarditis.
The 2025 ESC guideline emphasizes a presentation-driven approach to inflammatory myocardial and pericardial syndromes, with distinct clinical pathways for chest pain, heart failure, arrhythmia, and fulminant disease.
Red Flags
Features that should increase concern for clinically significant myocardial involvement include:
syncope
ventricular arrhythmia
high-grade AV block
new LV or RV dysfunction
acute heart failure
persistent or rising troponin
hemodynamic instability
cardiogenic shock
The more the presentation moves away from isolated chest pain/ACS and toward arrhythmia, conduction disease, ventricular dysfunction, or shock, the more urgently myocarditis should move up the differential.
What Changes Management?
Uncomplicated pericarditis without high-risk features
Many patients can be managed with anti-inflammatory therapy and appropriate follow-up.
Evidence of myocardial involvement
Troponin elevation, ventricular dysfunction, arrhythmia, or conduction disease should broaden the evaluation and generally lower the threshold for admission and advanced cardiac assessment.
Hemodynamic instability or cardiogenic shock
Think fulminant myocarditis. These patients may require aggressive hemodynamic support, advanced imaging, endomyocardial biopsy in selected cases, and early involvement of a center capable of mechanical circulatory support.
Pericardial effusion or tamponade physiology
Use echocardiography or POCUS to identify the effusion and assess the physiology. Tamponade is addressed separately later in this guide.
A normal bedside echocardiogram does not exclude myocarditis. POCUS can detect major dysfunction, effusion, or alternative pathology, but it is not a rule-out test for myocardial inflammation.
Common Pitfalls
Do not label all diffuse ST elevation as uncomplicated pericarditis.
Do not assume a normal bedside echo excludes myocarditis.
Do not dismiss unexplained tachycardia, ventricular arrhythmia, or new AV block in a patient with recent viral symptoms or chest pain.
Do not use troponin elevation alone to distinguish ACS from myocarditis.
Do not overlook the patient whose initial presentation is mild but whose clinical trajectory is worsening.
Related ECG STAT & Suggested Reading
Acute Pericarditis (ECG STAT)
STEMI vs. Acute Pericarditis: DDx (ECG STAT)
Diffuse ST Segment Elevation: DDx (ECG STAT)
2025 ESC Guidelines for the Management of Myocarditis and Pericarditis
Schulz-Menger J, Imazio M, et al. 2025 ESC Guidelines for the Management of Myocarditis and Pericarditis. European Heart Journal. 2025;46:3952–4041. PMID: 40878297.
This is the primary contemporary reference for this section. It is the first ESC guideline to address myocarditis and pericarditis together and provides a comprehensive framework for diagnosis, risk stratification, multimodality imaging, biopsy, treatment, and follow-up across the spectrum of inflammatory myocardial and pericardial syndromes.
[Read the full guideline] · [View on PubMed]
Myopericardial syndromes can range from benign-appearing chest pain to fulminant cardiovascular collapse. The next diagnosis is defined not by inflammation alone, but by obstructive physiology: cardiac tamponade.
End of this Section. Jump back to Top for section menu , or continue reading…
Cardiac Tamponade
Cardiac tamponade is physiology, not simply the presence of pericardial fluid.
A relatively small effusion that accumulates rapidly can cause severe hemodynamic compromise, while a much larger chronic effusion may be tolerated without tamponade. The rate of accumulation, pericardial compliance, intravascular volume, and intracardiac pressures all matter.
Think about tamponade early in unexplained shock. Do not wait for the full textbook picture.
The classic Beck triad of hypotension, jugular venous distention, and muffled heart sounds is insensitive. The ECG may show sinus tachycardia, low voltage, or electrical alternans, but none of these findings is sensitive enough to exclude a significant effusion or tamponade.
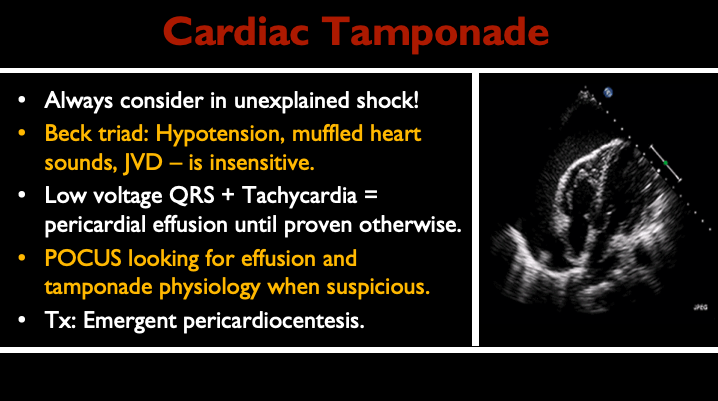
The ECG clue I want you to remember is low voltage plus otherwise unexplained sinus tachycardia. This is not specific enough to diagnose pericardial effusion by itself, but in the right clinical context it should immediately raise concern.
Low voltage is a clue. Tachycardia adds urgency. POCUS connects the ECG to the physiology.
Case: Low Voltage, Tachycardia, and a Changing Rhythm
Step 1: The Initial ECG
A 60-year-old man presents with chest and abdominal discomfort. During the examination, a change in rhythm is noted on the monitor.
Take a moment to review the initial ECG. What stands out?
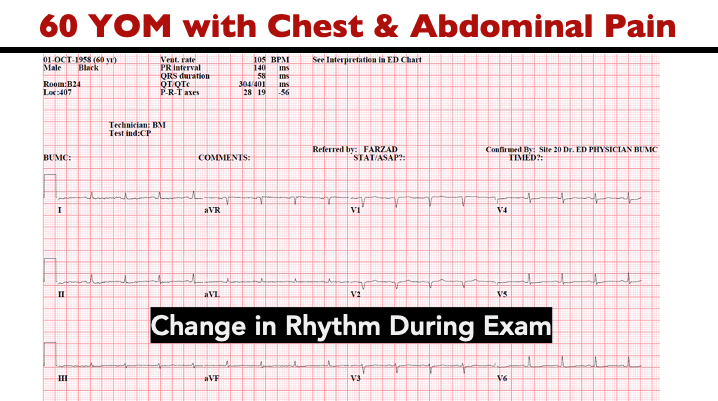
-
The ECG demonstrates low QRS voltage.
Low voltage is not a diagnosis. It is a clue that should trigger a differential and be interpreted in the context of the patient’s physiology.
What is Low QRS Voltage?
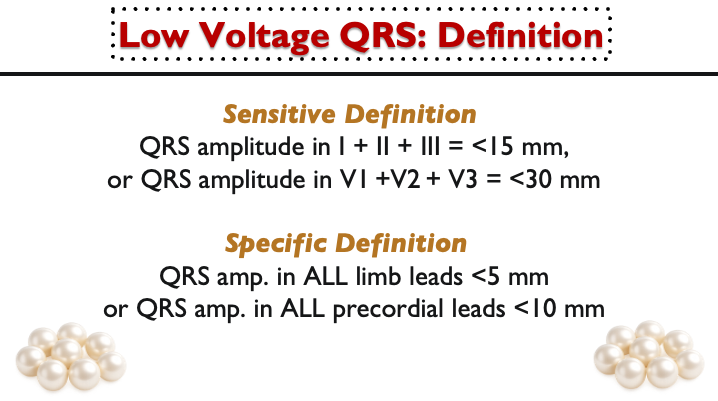
The conventional definition of low voltage is:
<5 mm in all limb leads, and/or
<10 mm in all precordial leads
The important question is not simply whether voltage is low. It is:
Why is the voltage low in this patient?
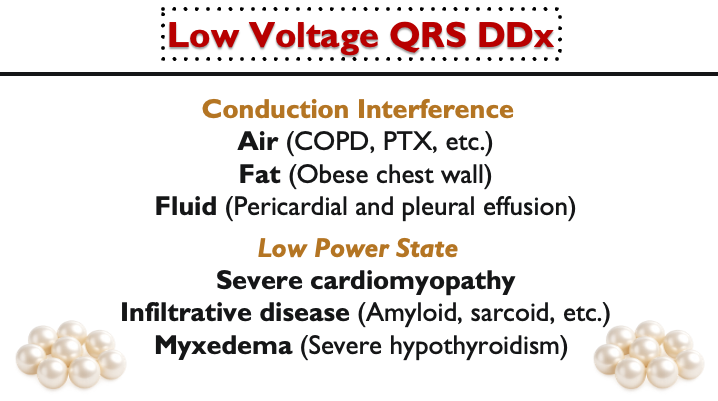
A practical differential is to ask whether something is interfering with electrical transmission or whether the heart itself is generating less electrical activity.
Conduction interference
Air — COPD, pneumothorax
Fat — obesity or increased chest-wall tissue
Fluid — pericardial or pleural effusion
Low-power states
severe cardiomyopathy
infiltrative disease
profound hypothyroidism or myxedema
The ECG gives you the abnormality. Your job is to fit the differential to the patient.
Step 2: The Rhythm Changes
The rhythm change on the monitor prompted a repeat ECG.
What has changed?
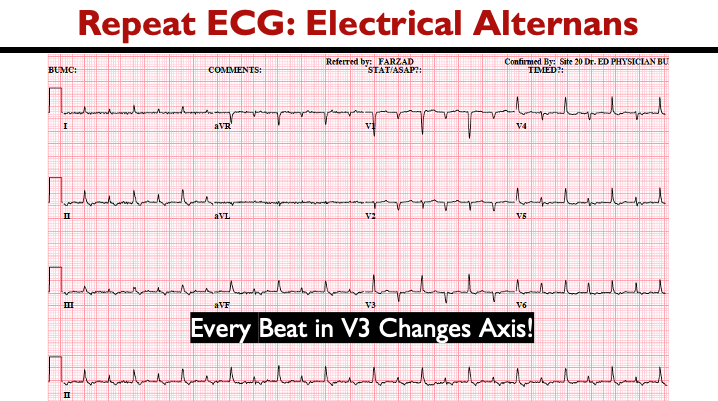
-
This is electrical alternans: beat-to-beat variation in QRS amplitude, axis, or both.
In a large pericardial effusion, the heart may move within the fluid-filled pericardial space, altering its spatial relationship to the recording electrodes.
Electrical alternans is an important clue when present, but it is insensitive and should never be required before considering tamponade.
Step 3: Look at the Heart
In a patient with hypotension, tachycardia, low voltage, and electrical alternans, bedside cardiac ultrasound should happen early.
The ECG created the suspicion. POCUS exposed the mechanism.
In tamponade, the key question is not simply whether fluid is present. The question is whether the effusion is producing clinically important hemodynamic compromise.
Tamponade is a clinical and physiologic diagnosis supported by imaging—not an ultrasound finding in isolation.
Take-Home Pearls
Low voltage plus otherwise unexplained sinus tachycardia should raise concern for a significant pericardial effusion in the right clinical context.
Electrical alternans is a useful clue when present, but it is insensitive.
Do not wait for Beck triad.
Do not wait for pulsus paradoxus.
Use POCUS early in unexplained shock.
Do not wait for the classic findings to become complete before acting on concerning physiology.
Common Pitfalls
Do not equate every pericardial effusion with tamponade.
Do not exclude tamponade because Beck triad is incomplete.
Do not wait for electrical alternans.
Do not interpret POCUS findings in isolation from the patient’s hemodynamics and clinical state.
Do not delay drainage in an unstable patient with convincing tamponade physiology.
Related ECG STAT & Suggested Reading
ECG in Pericardial Effusion (ECG STAT)
Low Voltage QRS: DDx (ECG STAT)
Pericardial Tamponade (ECG STAT)
The Diagnosis of Pericardial Effusion and Cardiac Tamponade by 12-Lead ECG
Eisenberg MJ, de Romeral LM, Heidenreich PA, et al. Chest. 1996. PMID: 8697827.
This is the key paper for understanding the diagnostic value and limitations of low voltage and electrical alternans in pericardial effusion and tamponade.
Cardiac Tamponade
Appleton C, Gillam L, Koulogiannis K. Cardiol Clin. 2017. PMID: 29025544.
A strong contemporary review of tamponade physiology, clinical presentation, echocardiographic findings, and management.
2025 ESC Guidelines for the Management of Myocarditis and Pericarditis
Schulz-Menger J, Imazio M, et al. 2025 ESC Guidelines for the Management of Myocarditis and Pericarditis. European Heart Journal. 2025;46:3952–4041. PMID: 40878297.
This is the primary contemporary reference for this section. It is the first ESC guideline to address myocarditis and pericarditis together and provides a comprehensive framework for diagnosis, risk stratification, multimodality imaging, biopsy, treatment, and follow-up across the spectrum of inflammatory myocardial and pericardial syndromes.
[Read the full guideline] · [View on PubMed]
The tamponade case brings together the central themes of this guide: recognize instability, use the ECG and POCUS as complementary tools, and act before the full textbook picture becomes obvious.
The final step is to bring everything together into a practical framework for the unstable chest pain patient.
End of this Section. Jump back to Top for section menu , or continue reading…
First Minutes: The Unstable Chest Pain Patient
When a patient with chest pain is unstable, the first question is not:
What is the final diagnosis?
It is:
What can kill this patient in the next few minutes, and is there anything I can treat immediately?
The unstable patient should move out of a routine chest-pain pathway and into active resuscitation.
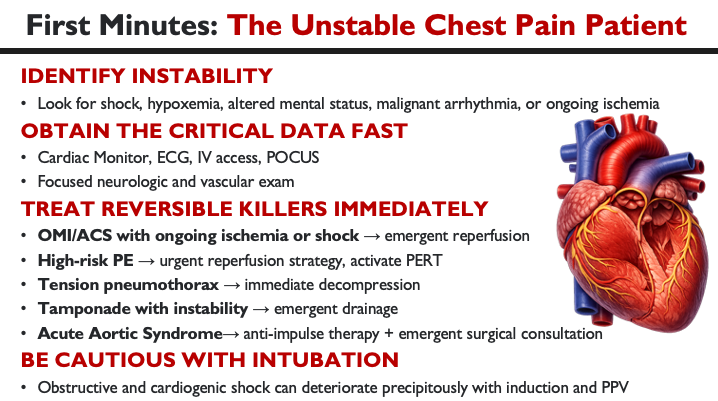
Identify Instability
Look for:
shock
severe hypoxemia
altered mental status
malignant arrhythmia
ongoing ischemia
These findings change the tempo of care. The more unstable the patient is, the less time there may be for complete diagnostic certainty before treatment begins.
Get Critical Data Fast
Obtain the information most likely to change immediate management:
cardiac monitor
ECG
IV access
early focused POCUS when appropriate
focused neurologic and vascular examination
POCUS can rapidly identify a large pericardial effusion, severe RV strain, major LV dysfunction, or another cause of shock. It should answer a focused clinical question rather than become an unfocused search for every possible abnormality.
In an unstable patient, the most useful test is the one that changes what you do next.
Treat Reversible Killers Immediately
OMI / ACS with ongoing ischemia or shock
→ Emergent reperfusion pathway
High-risk pulmonary embolism
→ Urgent reperfusion strategy; activate multidisciplinary PERT team when available
Tension pneumothorax
→ Immediate decompression
Tamponade with instability
→ Emergent drainage
Acute aortic syndrome
→ Anti-impulse therapy and emergent specialty consultation when indicated
Do not wait for perfect diagnostic certainty when the physiology and available evidence already justify immediate action.
Be Cautious With Intubation
Patients with obstructive or cardiogenic shock can deteriorate precipitously after induction, loss of sympathetic tone, and initiation of positive-pressure ventilation.
An airway may be necessary, but it is not benign.
Whenever possible:
understand the underlying physiology first
optimize hemodynamics before induction
anticipate peri-intubation cardiovascular collapse
have vasopressor support ready when appropriate
treat the reversible cause as early as possible
The airway is not always the first problem to solve. Sometimes the physiology has to be treated first.
Common Pitfalls
Do not let a routine chest-pain workup delay active resuscitation.
Do not wait for every laboratory result before acting on obvious ischemia, obstructive shock, or another immediately reversible killer.
Do not assume intubation will automatically improve an unstable patient.
Do not ignore the focused neurologic and vascular examination when acute aortic syndrome remains possible.
The Final Mental Model
The entire guide can be reduced to three questions:
1. What dangerous diagnosis could plausibly explain this presentation?
2. What is the pretest probability?
3. Is there anything here that cannot safely wait?
The goal is not to test every patient for every rare disease. It is to recognize who is genuinely at risk, use testing intelligently, reassess when the story changes, and act early when delay may be catastrophic.